Diet and poverty: Mind over money?
Obesity is popularly linked with
low-income groups and with a low socio-economic status (SES). This relationship
is frequently explained by a lack of money, a lack of understanding of healthy
nutrition, a general disdain for healthy eating and both isolation from
supermarkets and proximity to convenience and fast food outlets. I won’t argue
with this except to say that while obesity is more prevalent in low SES, there
are a lot of fat judges, mayors, prime ministers, presidents elect,
ex-sportsmen, doctors, nurses and others for whom the putative drivers of
obesity in poverty are generally absent. New research[1]
on obesity and SES has recently been published by scientists from Singapore’s
A*STAR and published in the prestigious journal, The Proceedings of the
National Academy of Sciences. The key question they asked was thus: Irrespective of your true SES, if you were made to think you were of a low SES, would that influence your
food habits?
They started their thinking process
with reference to the animal kingdom where in any social organisation, those
that are marginalized for whatever reason (too slow, too weak, too fussy), also
tend to overeat and gain weight. This might be a precaution for survival in the
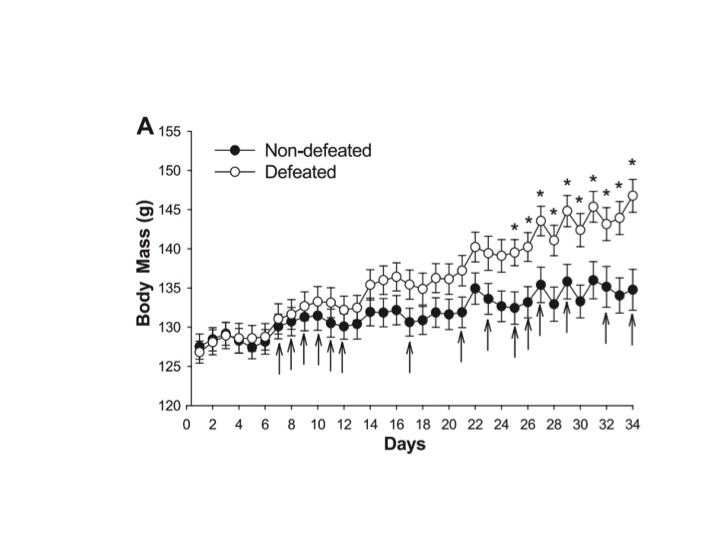
event that they might one day be in fact ousted from the group. They cite a
hamster study where a smallish hamster living in harmony with other small
hamsters is placed alone in a cage into which a larger hamster is admitted. The
latter will assert itself as dominant within less than a minute and the “defeated” smaller hamster is left to sulk.
The plot of body weight over time comparing those hamsters subject to defeat
against those spared this ignominy shows that the defeated hamsters,
stigmatized and “psychologically” marginalised, get fatter.
Against that background from the
animal kingdom of which the hamster data is merely illustrative of so many such
studies, they set out to study if an “imagined” low SES could alter food
habits.
The human volunteers were placed in
a private room and the study was conducted in what were effectively laboratory
conditions. They were shown a ladder with the following instructions:
Think of this ladder as
representing where people stand in Singapore. Now, please compare yourself to the
people at the very top of the ladder. These are the people who are the best
off—those who have the most money, most education, and most respected jobs. In
particular, we’d like you to think about how YOU ARE DIFFERENT FROM THESE
PEOPLE in terms of your own income, educational history, and job status. Where
would you place yourself on this ladder relative to these people at the very
top? Please select the number that corresponds to the rung where you think you
stand in relation to these people.
A second group was similarly treated but they compared
themselves to people at the bottom of the ladder: poor, less education and
rotten jobs. To emphasise the mental induction of subjective higher or lower
SES, subjects had to write down in detail how a conversation might go with the
group above or below themselves and to suggest how such a conversation might
flow. Now, suitably indoctrinated into a feeling of subjective high or low SES,
the experiments began and the easiest way to communicate the studies is to simply
focus on the results.
- When
asked to select the foods they might be subsequently included in a meal,
those who subjectively thought of themselves as lower SES, chose higher energy
dense foods and overall indicated an intention to eat more calories than
those who were attuned to think of themselves as higher SES
- When
asked to rate foods according to descriptors such as pleasant (e.g.,
tasty, delicious, wonderful) and unpleasant (e.g., disgusting, nasty,
awful) those in the lower SES subjective state chose the higher energy
density foods as the most pleasant
- In a
third study, the subjects viewed a short documentary video while freely
eating three snacks (potato chips, M&M candies, and California
raisins) from separate bowls. Those with the lower SES frame of mind ate
more calories and they more or less favoured the chips and M&Ms over
the raisins.
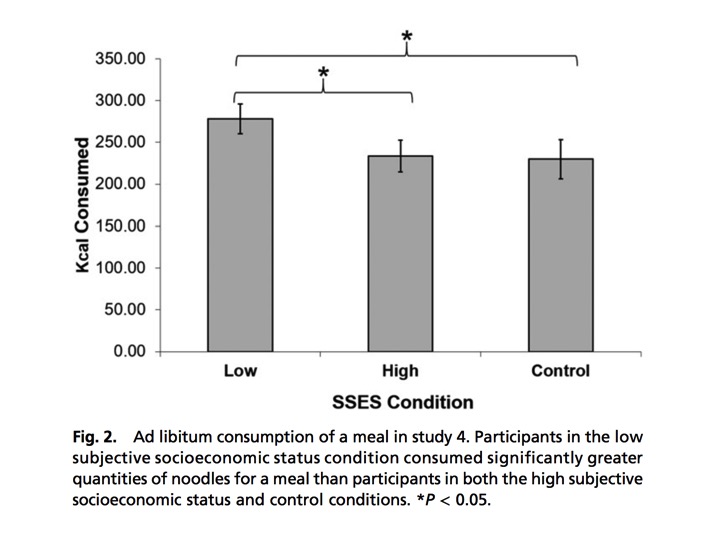
- Finally, the
subjects were given access to a meal in the form of noodles and asked to
eat to appetite. For completeness, a control group who did not take part in
the imagined SES ranking exercise was included. The outcome showed that
those who subjectively rated themselves as lower SES ate significantly
more then the other two groups.
These studies were carefully
designed and the analysis took statistical account of all key variables (age,
gender, weight etc.) including the actual SES of the subjects. The results could
be interpreted thus: When induced to think they are of a low SES, people
overeat because that’s what they think those of low SES actually do. However,
there are a few reasons to downplay this potential explanation. First, each
experiment involved different volunteers so there could be no sense of
training. Secondly, food was not portrayed as a central element of the study
but rather the self-imposition of a state of mind. Finally, and most
importantly, those induced to imagine themselves as low SES, were comparing
themselves to those at the top of the social ladder who were the economic
elite.
So, once again, we see what we
refer to as the “mind” playing a driving role in one of nature’s most powerful
biological drives, the drive to eat[2].
[1] Cheon BK & Hong Y-Y (2016) Mere experience of low
subjective socioeconomic status stimulates appetite and food intake Proceedings
of the National Academy of Sciences (Early edition) www.pnas.org/cgi/doi/10.1073/pnas.1607330114
[2] Mind over matter: Perceived time as opposed to real
time on blood glucose in type 2 diabetes: Blogged October 14th 2016